
The Limits of Stability (LOS) is perhaps the most used protocol in the literature for balance assessment in a dynamic task. It quantifies the ability to intentionally displace the center of gravity to the patient’s stability limits without losing balance. This protocol provides information regarding voluntary motor control, which also helps screening fall risk in elderly people [1].
- How is it done?
This protocol measures several movement characteristics in 8 different directions – front, forward/right, right, backward/right, backward, backward/left, left, and forward/left (Figure 1). The patient controls the blue point in real-time with its center of pressure (COP), and must:
- Hold in center until the target outlined changes color to orange (or hear a beep signal).
- As soon as it happens, move the blue point as quickly and as straight as possible towards the target, without losing balance.
- Stay in the reached position until the timer ends (8 seconds).
- Return to the center position.
- Repeat for the other directions.
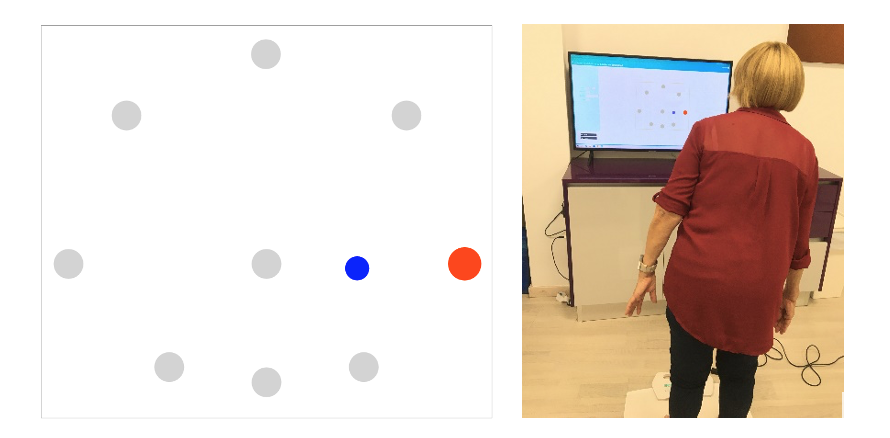
Figure 1 – Interface of Limits of Stability protocol.
The distances of the limits of stability targets are calculated according to the height of the patient’s center of gravity. These distances are calculated at 100% of the theoretical limits of stability, i.e., 8° left, right and front, and 4.5° back (Figure 2). During the leaning movement, the patient should be in a comfortable stance, without lifting the feet, with their body rigid (without rotations or hip movements). In case the patient cannot reach the orange target, they must remain in the reached position (towards the target).

Figure 2 – Theoretical boundaries of the limits of stability.
- Measures calculated
After performing the eight directions of the protocol, the trace of the center of pressure appears (Figure 3), as well as the following values:
- The reaction time (RT) is the time between the indication to move (2 seconds after clicking the Start button the color of the target changes to orange) and the first movement of the patient, in seconds.
- The endpoint excursion (EPE) is the distance from the first attempt to reach the orange target, expressed as a percentage of LOS. The end of the first attempt is considered the point at which the initial movement towards the goal ceases.
- The maximum excursion (MXE) is the maximum distance reached during the 8 seconds trial, expressed as a percentage of LOS.
- The movement velocity (MVL) is the distance travelled by the center of pressure, between 5% and 95% of the first attempt, divided by the elapsed time (°/s).
- The directional control (DCL) is the percentage of movement in the intended direction minus off-axis movement during the first attempt.
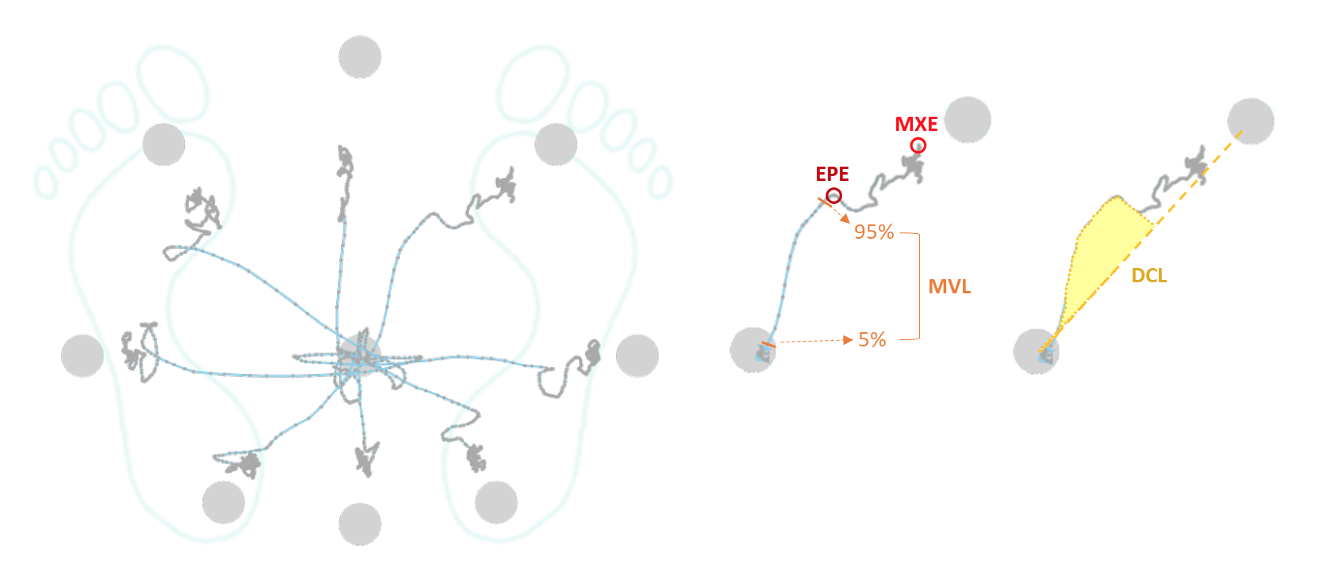
Figure 3 – Example of the COP trace during the LOS protocol, with illustration of the parameters calculated for the forward/right direction.
These values are calculated for each direction, and then the mean for each cartesian axis (front, back, right, left) and composite (mean of all directions) are presented along with the normative data for the patient age (Figure 4).
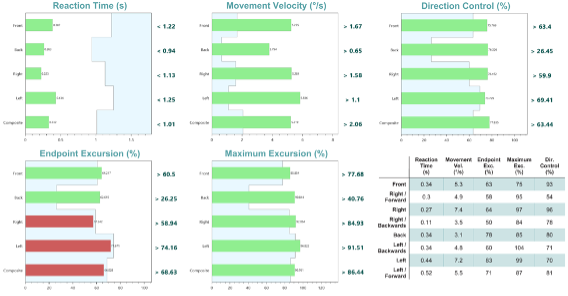
Figure 4 – Example of the results section for the LOS clinical report.
- Significance
The ability to voluntarily move the center of pressure within the limits of stability boundaries is fundamental for several functional tasks associated with activities of daily living (ADLs). With this protocol it is possible to assess the voluntary motor function, being appropriate for patients with central nervous system pathologies and peripheral neuropathic disorders, older adults with mobility impairments, and athletes interested in rapid movement reactions and direction changes. Kanekar, N. and Aruin, A. S. [2] used this protocol to investigate balance control differences between multiple sclerosis (MS) patients and healthy individuals. They found that the MS group had smaller limits, showed on the endpoint and maximum excursion values. In addition, there have been some studies about the correlation between ankle strength [3] and the limits of stability test, particularly the front-back maximum excursion. Also, Willems, T. M. et al. [4] demonstrated that low value of directional control was one of the parameters that could help predict an ankle injury.
Thus, results outside the normative values can be representative of a voluntary motor impairment, which can be influenced by several factors, such as biomechanical limitations, central movement disorders, sensory awareness, and fear [5]:
- Low values in direction control, maximum or endpoint excursion are indicative of limited range of motion, weakness, and other musculoskeletal deficiencies.
- Low movement velocity values are indicative of neuromuscular deficiencies caused by stroke, Parkinson’s disease, among other age-related disorders.
- Low reaction time values are indicative of cognitive deficits, fear of falling, and anxiety, often due to aging.
- Patients with acute symptoms of dizziness may be afraid to approach the limits of stability, showing results with values outside the normative values for all parameters.
Results within the normative values are indicative of good voluntary motor control and adequate proprioception of the lower limbs, as well as the range of motion and strength for mobility.
It is also important to point out that balance assessment using the limits of stability protocol allows objective measurement, that is reproducible, practical, and reliable, allowing comparison and progress monitoring after rehabilitation.
You may also like read about 12 Protocols for Balance Assessment with force/pressure plate.
>>>> Check our solutions and ask now for a quotation
Cláudia Tonelo
Sensing Future Technologies
Bibliography
[1] T. Bulat et al., “Effect of a group-based exercise program on balance in elderly,” Clin Interv Aging, vol. 2, no. 4, pp. 655–660, 2007, doi: 10.2147/cia.s204.
[2] N. Kanekar and A. S. Aruin, “The Role of Clinical and Instrumented Outcome Measures in Balance Control of Individuals with Multiple Sclerosis,” Multiple Sclerosis International, vol. 2013, pp. 1–10, 2013, doi: 10.1155/2013/190162.
[3] I. Melzer, N. Benjuya, J. Kaplanski, and N. Alexander, “Association between ankle muscle strength and limit of stability in older adults,” Age and Ageing, vol. 38, no. 1, pp. 119–123, Nov. 2008, doi: 10.1093/ageing/afn249.
[4] T. M. Willems, E. Witvrouw, K. Delbaere, N. Mahieu, L. De Bourdeaudhuij, and D. De Clercq, “Intrinsic Risk Factors for Inversion Ankle Sprains in Male Subjects: A Prospective Study,” Am J Sports Med, vol. 33, no. 3, pp. 415–423, Mar. 2005, doi: 10.1177/0363546504268137.
[5] S. Clark and D. J. Rose, “Evaluation of dynamic balance among community-dwelling older adult fallers: a generalizability study of the limits of stability test,” Arch Phys Med Rehabil, vol. 82, no. 4, pp. 468–474, Apr. 2001, doi: 10.1053/apmr.2001.21859.3/ageing/afn100.